

GROWING CHILD AND YOUTH: DWARFISM IDIOPATHIC HYPOPITUITARY (GHD IN THE ABSENCE OF DEFECTS OR ORGANIC ANATOMY SET).
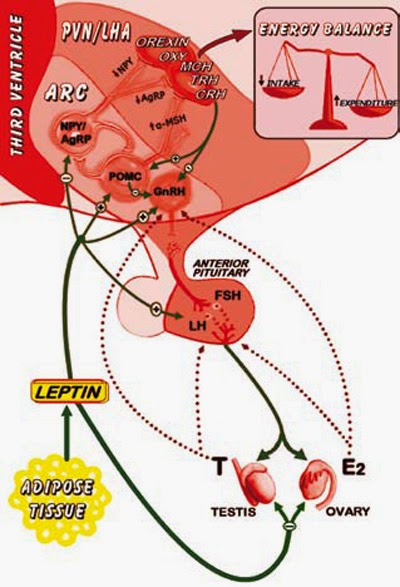

Patients with congenital GHD exhibit early onset of growth failure; this finding distinguishes those patients with GHD due to hypothalamic benign tumors, which usually present late growth failure. Even without a gonadotropin deficiency associated, patients with GHD treatment without often have delayed onset of puberty associated with its delayed bone age. However, with proper treatment with hGH rDNA onset of puberty occurs at the normal age. Patients with combined GHD and gonadotropin does not go through puberty even when the bone age reaches the puberty stage. The idiopathic hypopituitarism is usually sporadic, but can occur after a pattern of inheritance linked to X. The growth, the main characteristic of childhood and adolescence, has a similar pattern in most individuals. The genetic inheritance and the components of the GH-IGF axis are the factors that directly influence this process. GH produced in the pituitary, exerts its action on growth by regulating IGF system. IGFs (IGF-1 and IGF-2) are produced growth in most organs and tissues of the organism factors having autocrine, paracrine and endocrine actions on the intermediate metabolism, proliferation, cell growth and differentiation. They are associated with high specificity and affinity to a family of six binding proteins, called IGFBPs (IGFBP-1 to -6) that modulate their bioactivities. Most of the known actions of IGFs are exerted by binding to the type 1 receptor (IGF-1R). The pulsatile secretion of GnRH from the hypothalamus is a prerequisite for both the initiation and maintenance of the reproductive axis. The absent or diminished ability to secrete GnRH from the hypothalamus, or pituitary gland to secrete LH and FSH, leading to hypogonadotropic hypogonadism. This classification denotes an often irreversible condition that requires therapy. If the deficiency is limited pituitary gonadotropins, patients have a near-normal height for age. If patients have constitutional delay of adolescence they will be temporarily lower.

Dr. João Santos Caio Jr.
Endocrinologia – Neuroendocrinologista
CRM 20611
Dra. Henriqueta V. Caio
Endocrinologista – Medicina Interna
CRM 28930
Como saber mais:
1. O uso de GH rDNA para baixa estatura idiopática na prática clínica vai depender da sua eficácia na promoção do crescimento e do valor deste efeito para as famílias e médicos endocrinologistas - neuroendocrinologistas...
http://hormoniocrescimentoadultos.blogspot.com
2. A avaliação da altura e do peso de uma criança é um dos melhores indicadores de sua saúde geral e bem-estar...
http://longevidadefutura.blogspot.com
3. O crescimento anormal pode indicar a existência de doença subjacente na criança aparentemente normal. A detecção precoce e o diagnóstico de baixa estatura minimiza o impacto de qualquer condição de saúde subjacente e otimiza a altura final adulta...
http://imcobesidade.blogspot.com
AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO
DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA.
Referências Bibliográficas:
Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; Raben MS, Treatment of a pituitary dwarf with human growth hormone, J Clin Endocrinol Metab, 1958;18:901–3; Frasier SD, The not-so-good old days: working with pituitary growth hormone in North America, 1956–1985, J Pediatr, 1997;131:S1–S4; Hintz RL, The prismatic case of Creutzfeldt-Jacob disease associated with primary growth hormone treatment, J Clin Endocrinol Metab, 1995;80:2298–2301; Goeddel DV, Heyneker HL, Hozumi T, et al., Direct expression in Escherichia coli of a DNA sequence coding for human growth hormone, Nature, 1979;281:544–8; David A, Hwa V, Metherell LA, et al., Evidence for a continuum of genetic, phenotypic, and biochemical abnormalities in children with growth hormone insensitivity, Endocr Rev, 2011;32:472–7; Root AW, Kemp SF, Rundle AC, et al., Effect of long-term recombinant growth hormone therapy in children National Cooperative Growth Study, USA, 1985–1994, J Clin Endocrinol Metab, 1998;11:403–12; Cohen RN, Update on genetic regulation of pituitary development, Pediatr Endocrinol Rev, 2006;3:312–17; Richmond EJ, Rogol AD, Growth hormone deficiency in children, Pituitary, 2008;11:115–20; Ranke MB, Schweizer R, Lindberg A, et al., Insulin-like growth factors as diagnostic tools in growth hormone deficiency during childhood and adolescence: the KIGS experience, Horm Res, 2004;62:17–25; LM. G, Wilson DM, Is growth hormone stimulation testing in children still appropriate?, Growth Horm IGF Res, 2004;14:185–94; Frindik JP, Pituitary morphologic anomalies and magnetic resonance imaging in pediatric growth hormone deficiency, Endocrinologist, 2001;11:289–95; Wilson TA, Rose SR, Cohen P, et al., Update of guidelines for the use of growth hormone in children: the Lawson Wilkins Pediatric Endocrinology Society Drug and Therapeutics Committee, J Pediatr, 2003;143:415–21; Franklin SL, Geffner ME, Growth hormone: the expansion of available products and indications, Endocrinol Metab Clin North Am, 2009;38:587–611; Kemp SF, Growth Hormone Therapy: Dosing Considerations, Endocrinologist, 1996;6:231–7.
Contato:
Fones: 55 (11) 2371-3337 - 5572-4848 ou 9.8197-4706
Rua Estela, 515 - bloco D - 12º andar - conj 121 e 122 - Paraiso - São Paulo - SP - CEP 04011-002
email: vanderhaagenbrasil@gmail.com
Rua Estela, 515 - bloco D - 12º andar - conj 121 e 122 - Paraiso - São Paulo - SP - CEP 04011-002
email: vanderhaagenbrasil@gmail.com
www.vanderhaagenbrazil.com.br
http://drcaiojr.site.med.br
http://dracaio.site.med.br
João Santos Caio Jr
http://google.com/+JoaoSantosCaioJr
Vídeo
http://youtu.be/woonaiFJQwY
Google Maps:
http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl=pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie=UTF8&ll=-23.575591,-46.650481&spn=0,0&t = h&z=17